The ER Is Not First Come, First Served (And Why That Matters)
If you’ve ever sat in an emergency department waiting room and thought, “I was here first, why is that person going in before me?” you’re not alone. It’s one of the most common frustrations patients have, and honestly, it makes sense. In almost every other part of life, order matters. You take a number (deli counter, anyone…), you wait your turn, and eventually your number is called.
The emergency department does not work like that. It cannot work like that. The ER runs on priority, not order.
*I’m going to explain it long form first, however, if you want to skip to a visual representation, scroll all the way down.*
Alright then, let’s begin. The moment you arrive to the ER, your visit begins. You’re registered quickly and brought into triage, where a highly trained registered nurse asks targeted questions to determine the nature and severity of your condition. This isn’t small talk. It’s rapid clinical decision-making. Within minutes, the nurse is forming a picture: Is this person stable? Is this chief complaint potentially life-threatening? How quickly does this person need care? How many resources will likely be required?
From that assessment, a severity score is created -formally or informally depending on the facility policy. The most common is called the Emergency Severity Index (ESI) score. Whether the ESI score is used, or another, that score determines where you go next. Not when you arrived. Not how long you’ve been waiting. Severity.
That’s why someone who walked in after you may be brought back immediately. It’s not preferential treatment. It’s prioritization of risk.
And here’s the part that’s often misunderstood: being asked to wait is not a bad sign. In many cases, it’s actually a good one (stay with me here…). Being sent back to the waiting room means that, based on the information you presented to the triage nurse -in his or her expertise-, your condition is stable enough to safely wait while the team focuses on higher-acuity patients.
Let me pause here for a second to cover three important things: 1. [As a patient], please don’t ever say “it’s quiet in here today” or a variation of that phrase. To an ER nurse, saying that is equivalent to the Titanic hitting the iceberg: things will, without fail, start going sideways. 2. ER staff are determined to get ALL patients seen & treated as fast as possible, thus, the waiting room may be “empty” because the staff have used every nook & cranny of space in the department so that patients aren’t sitting in the waiting room. 3. There’s a ‘back door’ in every emergency department where patients being escorted by EMS and police enter. You can’t see that entrance when you walk in, but it often accounts for A LOT of people arriving, most often with truly emergent conditions that require immediate attention.
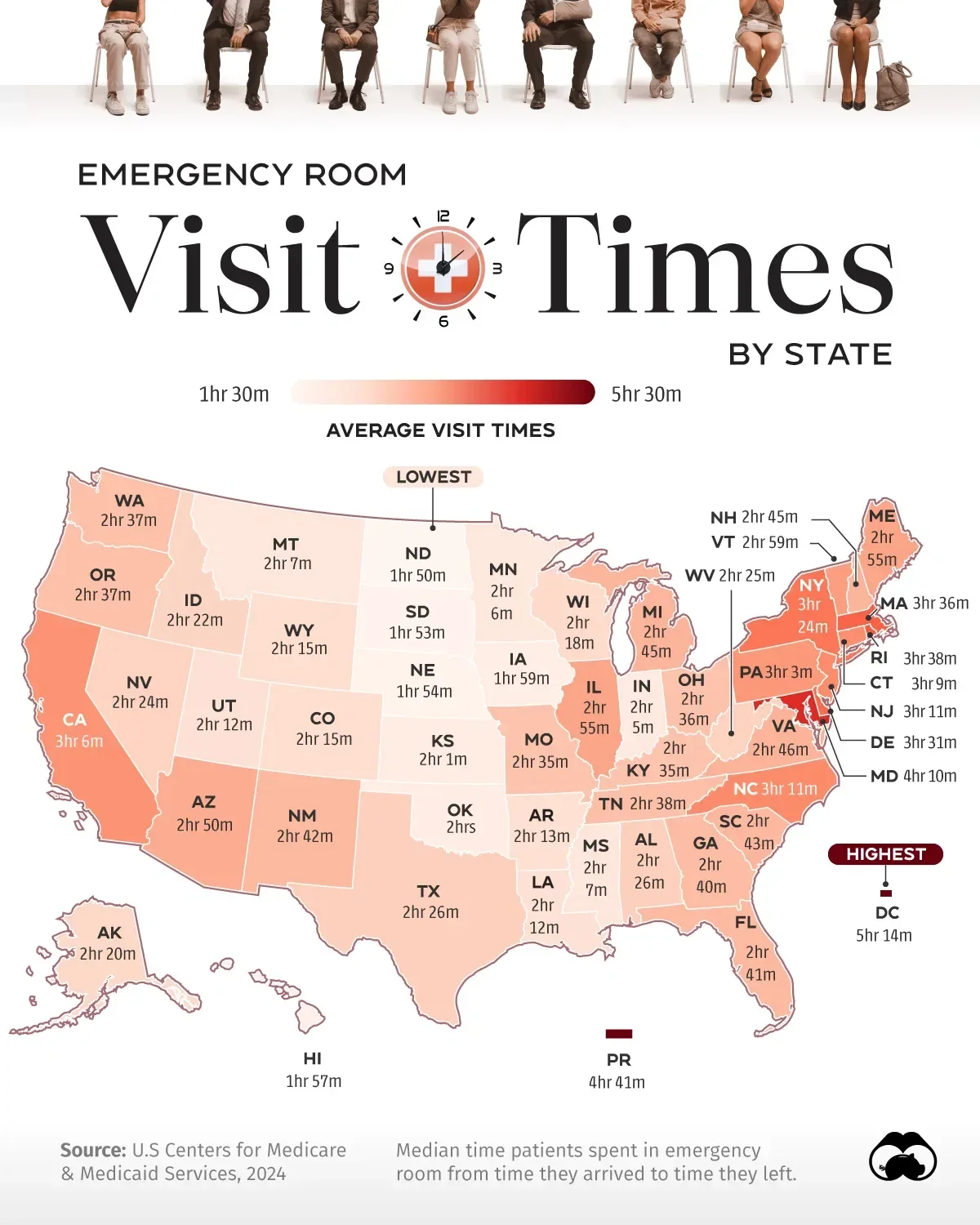
Ok, with that noted, let’s get back to your visit. Once you ARE brought back, the process moves in a structured way. You meet your care team; typically an emergency department physician (MD/DO) or physician assistant (PA) or nurse practitioner (NP/APN), a registered nurse (RN), and, in most ER’s, a patient care technician (PCT). From these interactions, initial testing begins. Bloodwork (or ‘labs’), imaging (xray, CT, or Ultrasound), and medications if needed. This is the “in progress” phase, which can take time, often one to three hours depending on what’s ordered. (As an aside, the average emergency department visit takes roughly 3.5 hours from arrival to discharge/admission. So, no, “this isn’t taking a long time” after being there for 1.15 hours).
During the aforementioned ‘in progress’ time, care doesn’t stop. There is ongoing reassessment by the RN and providers. Vital signs are repeated. Symptoms are re-evaluated. Treatments are adjusted. The team is constantly asking, “Is this patient getting better, worse, or staying the same?”
Eventually, results come back, decisions are made, and you move toward either discharge or admission. It’s a flow. Not a line.
That’s the key distinction. The emergency department is not a queue. It’s a dynamic system designed to identify and manage risk in real time. The ER simply makes that visible in a way that’s hard to ignore.
We like to believe that fairness means equal order. But in reality, fairness in high-stakes environments often means appropriate prioritization. So the next time you -or someone you know- sits in a waiting room feeling frustrated, it may help to reframe the situation.
You’re not being skipped. You’re being sorted.
And that system, imperfect as it may feel in the moment, is designed to do one thing above all else: make sure the sickest patients get care when they need it most. Because when you are truly on the emergent side of a situation, you want to receive care immediately!
That’s not just efficient. It’s necessary.
-Mitch
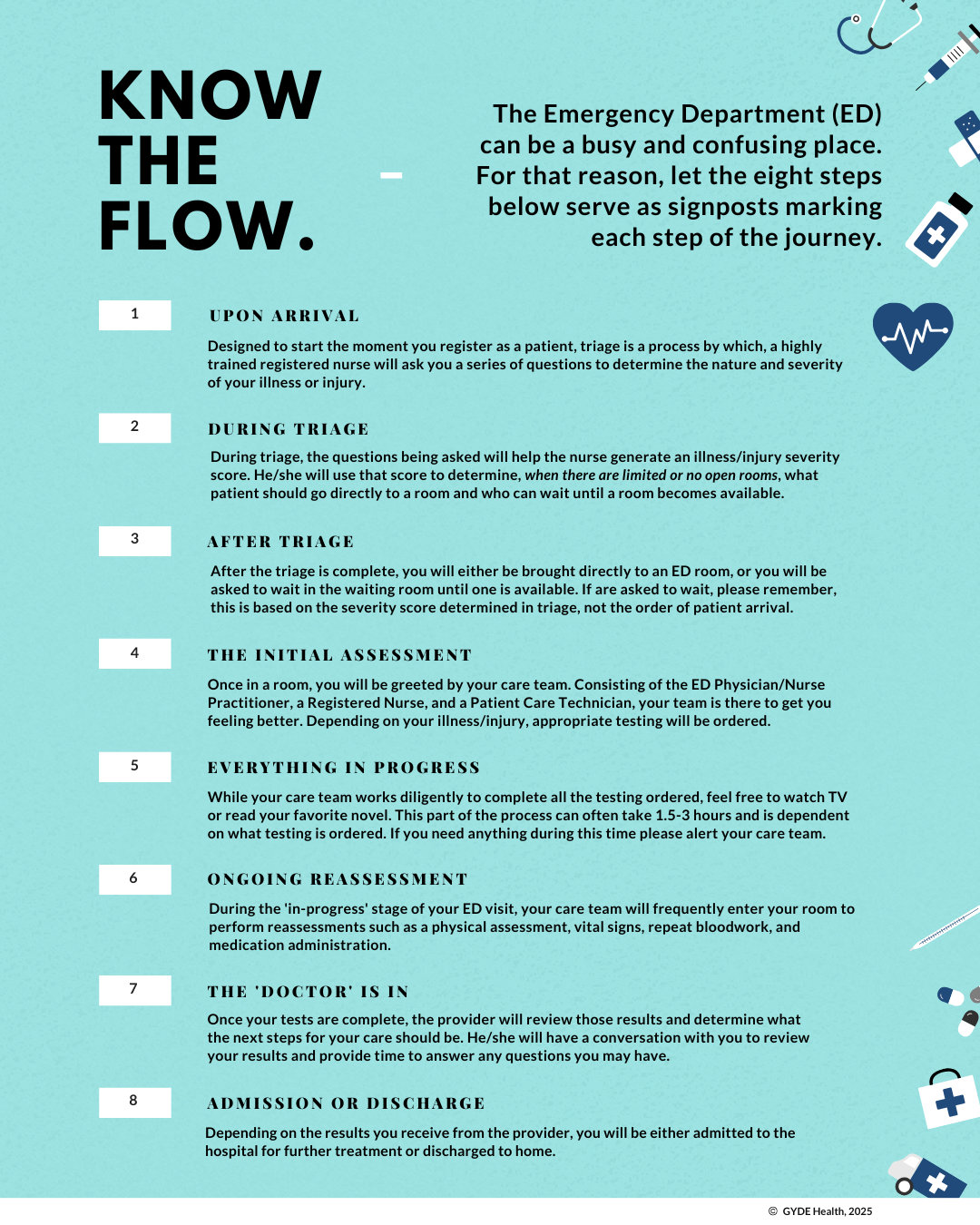
Before you assume the emergency department is “behind” or disorganized, it helps to understand what’s actually happening. The ER doesn’t operate like a line; it operates like a system. Every patient is assessed, prioritized, and managed based on severity, not arrival time. The visual walks you through the real flow of an emergency department visit, from the moment you arrive to the moment you leave -or get admitted. Once you see it, the experience makes a lot more sense.